|
|
|
Summer 2026 - Vol. 21, No. 2
EDUCATIONAL QUIZ FROM URGENT CARE
Ketogenic Diet-Associated Hypomagnesemia
Madeline Cingle, PA-C
Physician Assistant, Urgent Care Lebanon
Penn Medicine Lancaster General Health
CASE HISTORY
A 77-year-old male presents to an urgent care center with three days of intermittent dizziness, primarily positional. The episodes last 5-10 minutes, occurring when he is transitioning from lying to sitting; the episodes are most noticeable in the early morning. He denies syncope, chest pain, palpitations, dyspnea, headache, visual changes, focal neurological deficits, hearing loss, tinnitus, fever, or chills.
The patient reports initiating a ketogenic diet approximately three-and-a-half weeks ago, resulting in a 17-pound intentional weight loss from 212 pounds to 195 pounds. He reports adequate hydration.
His past medical history includes gastroesophageal reflux disease (GERD), hypertension, benign prostatic hyperplasia, chronic gout, arthritis, bladder cancer that is now in remission, and atherosclerosis of the aorta.
His regular medications include omeprazole, allopurinol, amlodipine-benazepril, red yeast rice, tamsulosin, tadalafil, a multivitamin, and simethicone.
The vital signs are notable for a blood pressure of 154/86 mmHg but otherwise are within normal limits. A neurological exam is unremarkable, and there is no evidence of orthostatic hypotension. A Dix-Hallpike maneuver reproduces dizziness without nystagmus, making benign paroxysmal positional vertigo less likely.
An electrocardiogram shows sinus rhythm with a first-degree atrioventricular block.
Given that there is a concern for electrolyte abnormalities in the setting of his recent ketogenic diet, a laboratory evaluation is obtained, revealing a critically low serum magnesium level of 0.8 mg/dL. The patient is immediately referred to an emergency department, where he receives intravenous magnesium replacement with rapid resolution of his symptoms. His borderline hypokalemia (initially 3.5 mmol/L) is also corrected.
He is discharged home with a prescription for oral magnesium supplementation and dietary counseling. He is encouraged to remain hydrated and to continue close outpatient laboratory follow-up with his primary care clinician, including a discussion of the role of his proton pump inhibitor and whether/how that should be reduced.
At the time he is discharged from the emergency department, the patient reports complete resolution of dizziness.
QUESTIONS
- What is the differential diagnosis for positional dizziness in an older adult?
- What electrolyte abnormalities are associated with ketogenic diets?
- What are the clinical manifestations of hypomagnesemia?
- What factors increase the risk of hypomagnesemia in patients following a ketogenic diet?
- How should severe hypomagnesemia be managed?
- What counseling should be provided to patients considering ketogenic diets?
ANSWERS
- The differential diagnosis for dizziness that increases with position change includes benign paroxysmal positional vertigo, orthostatic hypotension, dehydration, electrolyte abnormalities, medication side effects, cardiac arrhythmias, and central neurologic causes such as stroke or transient ischemic attack.1
- Ketogenic diets are associated with an increased risk for hypomagnesemia, hypokalemia, hyponatremia, hypocalcemia, and metabolic acidosis, particularly within the first four weeks of the diet.2 Hypomagnesemia is among the most common early-onset complications.
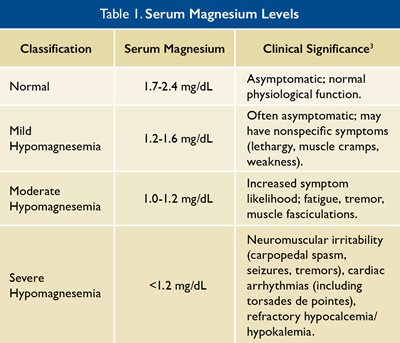
- Clinical manifestations of hypomagnesemia include dizziness, weakness, muscle cramps, tremors, neuromuscular irritability, and fatigue. Severe deficiency may lead to seizures, cardiac arrhythmias, torsades de pointes, and refractory hypocalcemia or hypokalemia (see Table 1).3
- Risk factors increasing the risk for hypomagnesemia include inadequate dietary magnesium intake, rapid weight loss, dehydration, renal magnesium wasting, concurrent hypokalemia or hypocalcemia, and medications such as proton pump inhibitors.4
- Severe or symptomatic hypomagnesemia should be treated with intravenous magnesium sulfate followed by oral supplementation.3 Coexisting electrolyte abnormalities must be corrected, and underlying contributors such as medications or dietary patterns should be addressed.3
- Patients should be counseled about the risks associated with rapid weight loss, that they should maintain adequate hydration, along with the need for routine electrolyte monitoring. Patients should be taught to recognize warning symptoms. Many patients will need magnesium supplementation and alternative dietary approaches if deficiencies occur.2,5
DISCUSSION
A ketogenic diet is characterized by high fat intake and marked carbohydrate restriction, inducing a state of ketosis that promotes rapid weight loss. 6 While effective for certain therapeutic indications and increasingly popular for weight management, this diet significantly alters electrolyte balance, particularly during early phases of initiation. 3,5
Hypomagnesemia is among the most frequently observed electrolyte disturbances associated with ketogenic diets. Dietary restriction of magnesium-rich foods such as whole grains, legumes, fruits, and certain vegetables contributes to inadequate intake. 3 Additionally, ketosis and associated diuresis may increase renal magnesium losses. Dehydration, commonly reported during early ketogenic dieting, further exacerbates electrolyte depletion. 2
Clinical recognition of hypomagnesemia is challenging due to its nonspecific symptoms, which may be misattributed to benign “keto flu.” Importantly, severe hypomagnesemia can lead to life-threatening cardiac arrhythmias and neurologic complications. 3 Magnesium deficiency also impairs parathyroid hormone secretion and action, leading to refractory hypocalcemia unless magnesium is corrected. 3
The concomitant use of proton pump inhibitors (PPIs) further increases the risk of profound hypomagnesemia. Long-term PPI use is associated with impaired intestinal magnesium absorption, making patients on both ketogenic diets and PPIs particularly vulnerable. 3,4
This case highlights the importance of understanding the dietary history in patients presenting with nonspecific dizziness or neuromuscular symptoms. Early laboratory evaluation, prompt treatment, and targeted counseling can prevent significant morbidity.
REFERENCES
1. Alla S, Rao MY, Aslam SM. Clinical profiles of elderly patients presenting with persistent dizziness. Ochsner J. 2020;20(3):218-224.
2. Kang HC, Chung DE, Kim DW, Kim HD. Early- and late-onset complications of the ketogenic diet for intractable epilepsy. Epilepsia. 2004;45(9):1116-1123.
3. Touyz RM, de Baaij JHF, Hoenderop JGJ. Magnesium disorders. N Engl J Med. 2015;373(19):1853-1863.
4. Perazella MA. Proton pump inhibitors and hypomagnesemia: a rare but serious complication. Am J Med Sci. 2013;345(3):171-174.
5. Dy ńka D, Rodze ń Ł, Rodze ń M, et al. The ketogenic diet is not for everyone: contraindications, side effects, and drug interactions. Ann Med. 2026;58(1):2603016.
6. Ahmad Y, Seo DS, Jang Y. Metabolic effects of ketogenic diets: exploring whole-body metabolism in connection with adipose tissue and other metabolic organs. Nutrients. 2024;16(10):1900.
|
|